Symptoms and Diagnosis
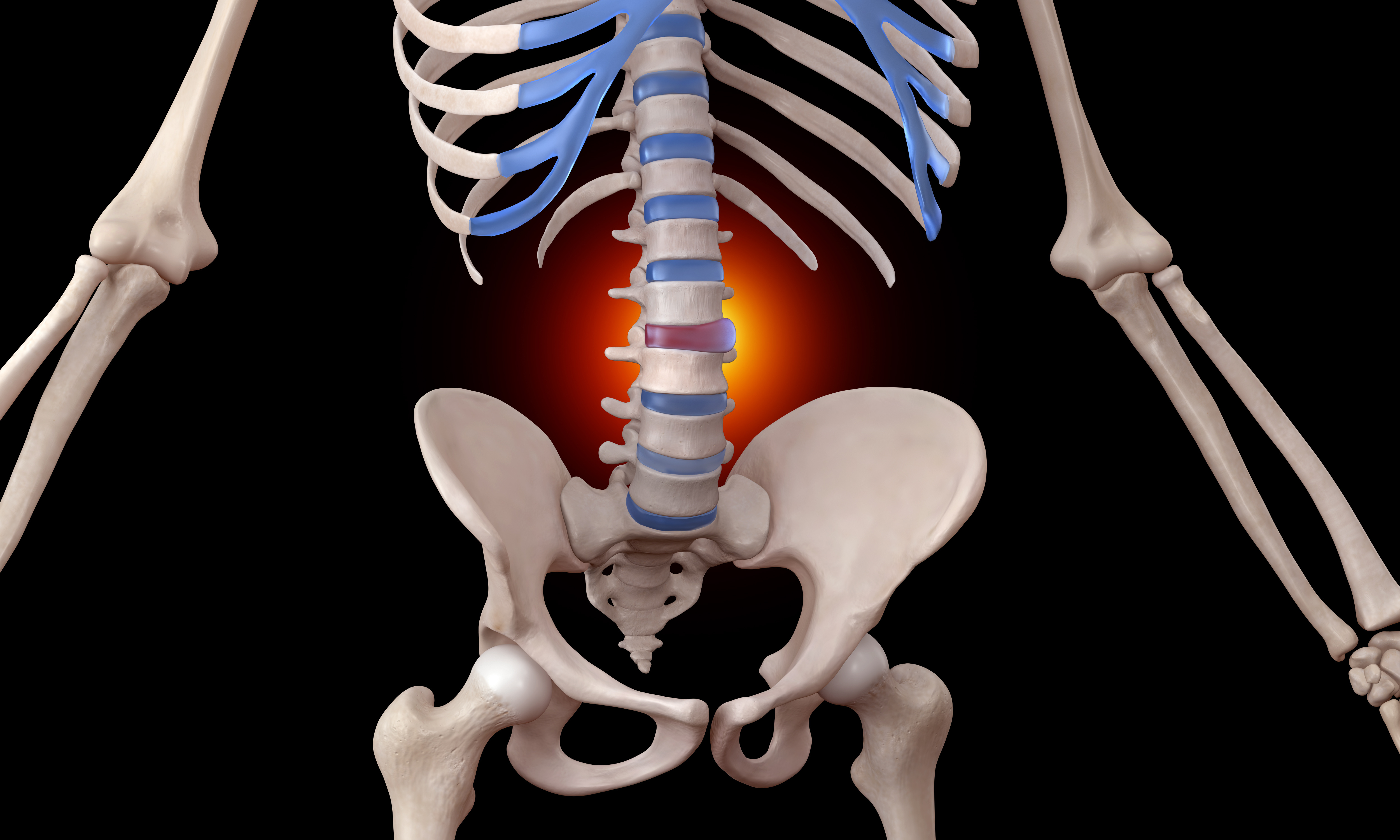
Lumbar disc herniations typically produce sciatica: pain radiating from the low back through the buttock and down the leg, often following a specific dermatomal pattern. An L4-L5 herniation commonly affects the L5 nerve root, producing pain along the lateral leg and dorsum of the foot. An L5-S1 herniation typically affects the S1 nerve root, radiating to the posterior calf and lateral foot. Cervical herniations produce neck pain with radiculopathy into the shoulder, arm, or hand.
Beyond pain, nerve compression can produce numbness, tingling, and in more severe cases, motor weakness-difficulty with foot dorsiflexion (foot drop) or grip strength, depending on the level. These neurological findings help localize the affected level even before imaging.
Diagnosis combines a detailed neurological examination with MRI, which reveals the disc morphology, the degree of neural compression, and any associated findings such as annular tears, facet arthropathy, or spinal stenosis. In my practice, I also use diagnostic musculoskeletal ultrasound during the physical examination to assess soft tissue structures in real time. Correlating clinical findings with imaging is essential-MRI alone does not tell us whether the herniation is the primary pain generator.
The Limitations of Conventional Herniation Treatment
Natural resorption occurs in many cases: Studies suggest that up to 60-80% of herniated discs show some degree of spontaneous resorption on follow-up imaging. The challenge is the interim period while waiting for resorption.
Epidural steroid injections can provide temporary relief by reducing perineural inflammation, but they do not promote annular healing, do not address the structural defect, and repeated use carries catabolic concerns. Oral medications manage symptoms but not pathology.
Microdiscectomy-the surgical removal of herniated disc material-is effective at decompressing the nerve root, but it removes tissue without repairing the annular defect. The recurrence rate for disc herniation after microdiscectomy ranges from 5-15%, precisely because the structural weakness in the annulus remains.
This is the gap that regenerative medicine addresses: promoting healing of the annular defect while managing acute nerve compression, treating both the symptom and the structural cause.
Dr. Crane's Regenerative Approach to Disc Herniation
My approach to disc herniation depends on the type, location, severity, and the patient's neurological status. Not every herniation is appropriate for regenerative treatment-and I am transparent about that.
For contained herniations (bulges and protrusions) with intact annular fibers, regenerative injection therapy can reinforce the annulus and promote repair of the weakened fiber layers. By delivering concentrated biological repair signals directly to the annular defect, we stimulate fibroblast proliferation and collagen synthesis. Over weeks, the annular fibers strengthen, and the disc becomes more structurally competent at containing the nucleus.
The supporting ligamentous structures around the herniated segment also require attention. When a disc herniates, the surrounding ligaments - the posterior longitudinal ligament, the interspinous and supraspinous ligaments - are often stretched or weakened. Regenerative treatment can stimulate repair in these ligaments, restoring tensile strength and improving segmental stability.
For larger herniations with significant nerve compression, I often combine regenerative treatment with targeted perineural injections to manage acute radicular pain while the biologic treatments take effect. The goal is to support the body through the acute phase while providing the biological resources for lasting structural repair.
Patients with progressive neurological deficits-worsening weakness, bowel or bladder changes-require urgent surgical evaluation. Regenerative medicine is powerful, but recognizing its limitations is as important as understanding its potential. I will refer for surgery when the clinical situation demands it.
What to Expect During Treatment
Treatment begins with a thorough diagnostic evaluation to confirm the herniation is the primary pain generator and to characterize the type and severity. If regenerative treatment is appropriate, we develop a phased protocol.
Initial treatment involves targeted regenerative injections to the annular fibers adjacent to the herniation under image guidance, with supportive treatment to the surrounding ligaments as needed. We monitor progress with clinical assessment and, when indicated, follow-up imaging to assess structural change.